Chapter 71: Upper Brachial Plexus Palsy
Avulsion of C5 C6 roots and/or Rupture (laceration) of their Combined Trunk
The compiler of these short notes thanks Drs. Raja Sabapathi the director of the plastic and microsurgical services and a hand surgeon at the Ganga hospital in Coimbatore a leading plastic surgery centre in India, his associate Hari Venkatramani who in turn was helped by Dr. Dalton Jerome. Equally valuable was the guidance given by Dr Mukund Thatte a plastic surgeon specialising in hand and brachial plexus surgery of Bombay hospital in Mumbai India who was helped by Dr. Amita Hiremath his associate.
The nature of accidents which cause injuries to the brachial plexus is described in detail in chapter 69. To revise this in short, any fall for example usually from a two wheeler where the ipsilateral shoulder is depressed and the neck is severely flexed laterally to the opposite side leads to this condition and as stated in the previous chapter more than fifty percent of such cases involve all roots and/ or trunks of the brachial plexus.(C5 to T1).Because of the acute angle at which the trunk of the of the upper roots(C5 C6) courses down the neck as compared to the lower roots and trunks the injury to this part of the brachial plexus is commoner than the rest in the remaining fifty percent of the cases particularly if the shoulder is in adduction at the time of the impact about 15 percent. In cases where the rider is thrown over the handle bars at the time of the impact and the shoulder is in abduction the lower roots and the trunks are more likely to be affected.
The avulsion of the C5 C6 roots or rupture(laceration) of the upper trunk lead to a paralysis of the supraspinatus and the infraspinatus (suprascapular nerve C5C6) the deltoid (the axillary nerve C5C6) the biceps brachii and the brachialis muscle (both supplied by the musculocutaneous nerve C5C6).

This mainly leads to absence of abduction and external rotation of the shoulder and inability to flex the elbow which can be improved a great deal by the existing methods of repair (Please see photographs at the end of the chapter before the atlas of the operative steps). The sensory loss on account of this condition occurs over the lateral surface of the shoulder and also involves the index finger and the thumb. The crisscrossing of the nerves within the brachial plexus is such that the sensory loss is usually not severe enough to cause trophic changes.
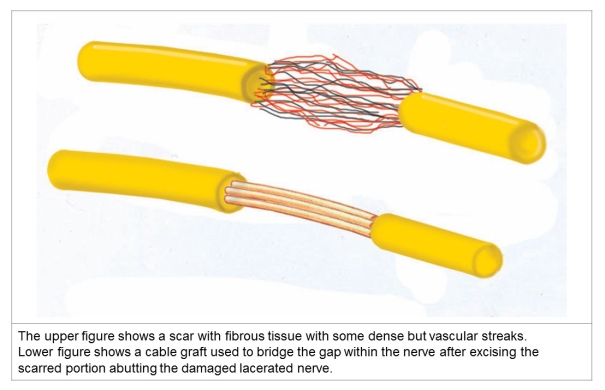
The modalities for radiological diagnosis to pin point if the injury involves avulsion of roots with or without a pseudo meningocele have been described in chapter 69. The rupture of the upper ensuing trunk and its severity may not be easy to diagnose completely preoperatively and is usually done intra-operative (Sunderland classification chapter 69). In case of a Post Ganglionic injury i.e. rupture intra-plexal repair of a ruptured common trunk of C5 C6 roots such as by excising a neuroma and approximation of the cut ends of the trunk without tension or bridging a ‘net nerve deficit’ by a nerve graft are performed if possible.

Photographs contributed by Dr. Raja Sabapathi and Dr. Hari Venkatramani, Coimbatore
A common source for the nerve graft is the sural nerve. Its anatomical course is reproduced below by way of a cadaveric dissection.

This repair helps towards rehabilitation of the other muscles around the shoulder girdle and helps to stabilise the shoulder joint in which the desired movements will occur with greater ease.
This repair also helps improvement in the sensations over the shoulder region and in the hand. However, the surgeon also aims to reinnervate the affected muscle (or muscles) near its hilum by a distal nerve transfer for more predictable results because the reinnervation is faster due to a much lesser distance that the process of reinnervation has to traverse.
The aim of these distal transfers done to rehabilitate a patient with C5C6 lesions are to restore abduction and external rotation of the shoulder and flexion at the elbow. While restoring the flexion at the elbow by reinnervating the biceps the action of supination also comes to be normalised because the biceps is an additional supinator at the radioulnar joint in addition to the supinator proper which is supplied by a branch of the radial nerve (Root Value C7 C8). This is however achieved only if the action of the paralysed biceps improves to over grade 4+. The restoration of the action of the biceps also helps the stabilisation of the shoulder joint.
The supraspinatus as well as the infraspinatus are reinnervated by the spinal accessory nerve (XI) harvested at the level of the middle fibres of the trapezius (The upper third of the Trapezius remains innervated) by joining it to the suprascapular nerve which arises from the upper trunk (C5C6).

The restoration of the abduction of the shoulder by the deltoid is achieved by reinnervating the anterior division of the axillary nerve (root valueC5C6 via the posterior cord) by the branch of the radial nerve to the long head of the triceps (root value C6C7C8) after it has been ascertained preoperatively that the triceps muscle is functional (at least MRC grade 4).

Figures photoshopped from Gray’s Anatomy
Flexion of the elbow is aimed to be restored by borrowing the antero-medial fascicle of the ulnar nerve (root value C8 T1) to reinnervate the branch to the biceps of the musculocutaneous nerve (root value C5C6) and additionally the central fascicle of the median nerve is used to reinnervate the branch of the musculocutaneous nerve to the brachialis. The use of the fascicles of the ulnar nerve were first described by Oberlin while the addition of the fascicles of the median nerve to the nerve to the brachialis was described by Susan Mackinnon.



All repairs are done without any tension and this is further confirmed by performing passive movements of the shoulder and elbow with the coaptation in view. Should there be any evidence that such movements are causing tension then the patient’s shoulder is immobilised in adduction for four weeks and the elbow is held at 135 degrees flexion, both are then slowly and progressively mobilised.

Photographs contributed by Dr. Raja Sabapathi and Dr. Hari Venkatramani, Coimbatore


Photographs contributed by Dr. Raja Sabapathi and Dr. Hari Venkatramani, Coimbatore

Pictures contributed by Dr. Mukund Thatte and Dr. Amita Hiremath, Mumbai.
The following pictorial atlas gives a step by step description of how the Brachial Plexus is explored.



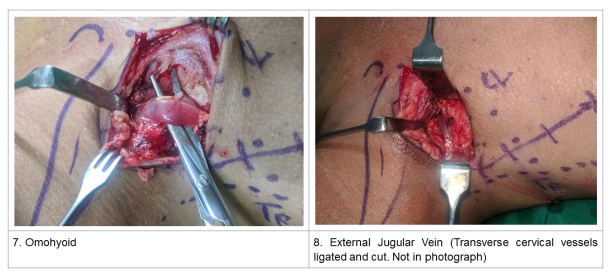





These pictures are contributed by Nayana Nayak, clinical associate of Mukund Thatte at the Bombay Hospital, Mumbai.
Notes: Teres minor is an important external rotator of the shoulder joint and has been specifically reinverted by some surgeons using the phrenic nerve, a motor branch of the triceps or the long thoracic nerve if it has escaped the effects of the injury to C5C6 nerves. This is done by re-innervating a branch of the lower subscapular nerve which supplies the teres minor muscle.
It is expected that exposure of the nerves in the upper arm will be included in the next chapter which will discuss injuries to the lower brachial plexus.

